Lots of long-term travellers go through malaria risk areas. Antimalarial medication comes at a cost and can cause side effects. Therefore, round-the-world (RTW) travellers wonder whether or not they should take it to protect themselves. In this article, we’ll give you all the necessary information to fully understand the risks associated with the areas you’re going to visit and the solutions to prevent malaria. Of course, this information is not medical advice. Only a doctor can advise you on whether or not to take antimalarial medication and on the options available.
Malaria is an infection spread by parasites that belong to the genus Plasmodium. Humans can become infected if they’re bitten by female Anopheles mosquitoes, which are themselves infected. They mostly bite between sunset and sunrise. Male mosquitoes don’t bite.
Malaria can’t be passed on from person to person, except in the case of pregnant women, who can infect their child.
Malaria symptoms usually start to appear between 8 and 30 days after becoming infected.
Symptoms include a high temperature, often accompanied by digestive problems, muscle pains, headaches, fatigue and a cough. Typical symptoms occur in the following alternating cycle: high temperature, shivering, cold sweats and severe sweating.
There are four types of malaria, each caused by a different parasite:
Malaria is mainly found in tropical regions.
Unlike dengue, the risk of malaria is much higher in rural or forest areas than it is in city centres. It decreases with altitude. Above 6,500 to 9900 feet (2,000 to 3,000 metres) the mosquitoes that spread the infection can no longer reproduce. The risk is also higher during periods of heavy rain and the following weeks.
Number of malaria cases per 1,000 population per country
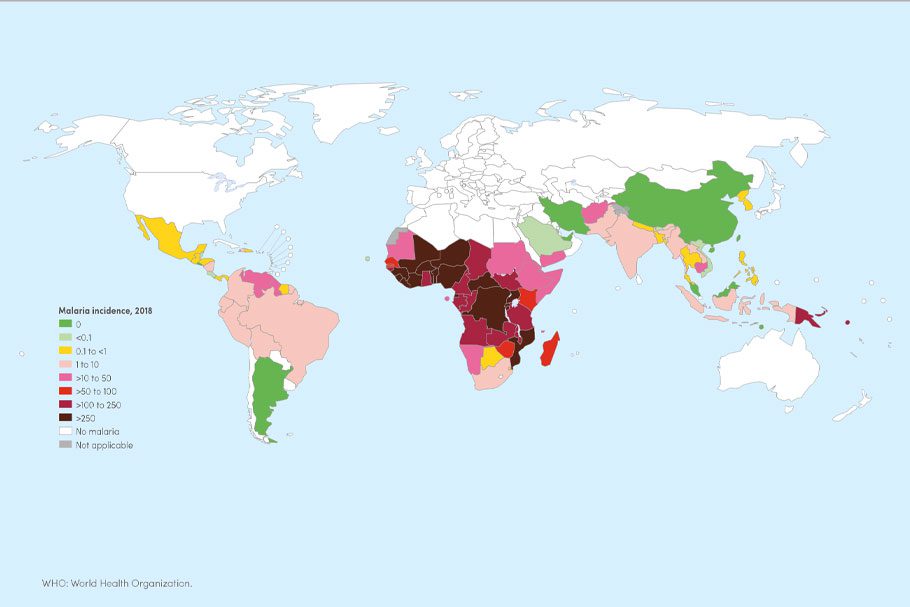
Source: World Health Organisation: World Malaria Report 2019 p.50
P. falciparum parasite prevalence in Africa
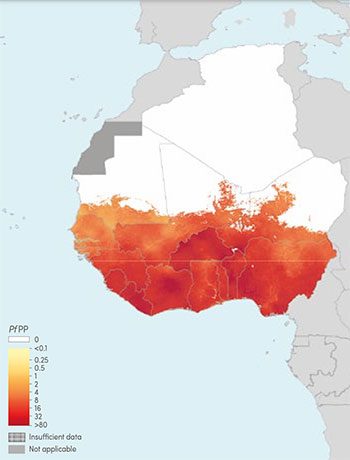
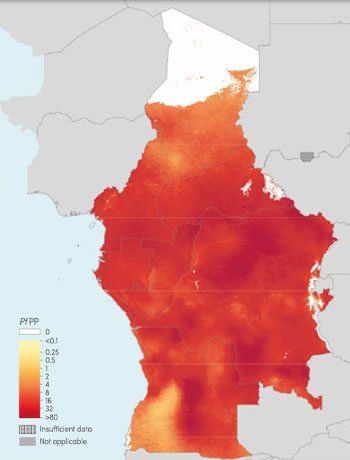
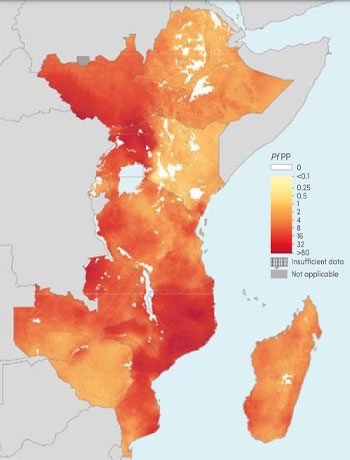
Source: World Health Organisation: World Malaria Report 2019 p.140, 142, 144
Number of malaria cases per 1,000 population in Latin America
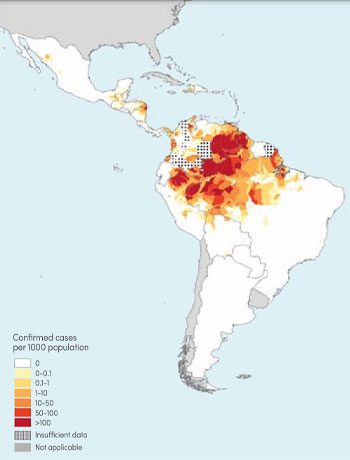
Source: World Health Organisation: World Malaria Report 2019 p.148
Number of malaria cases per 1,000 population in Asia
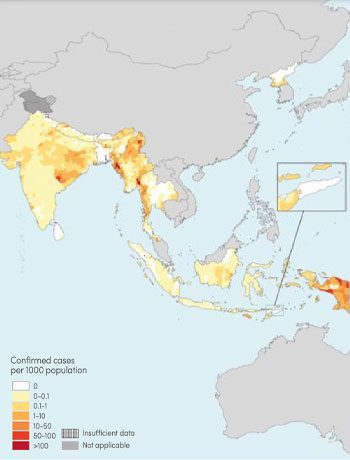
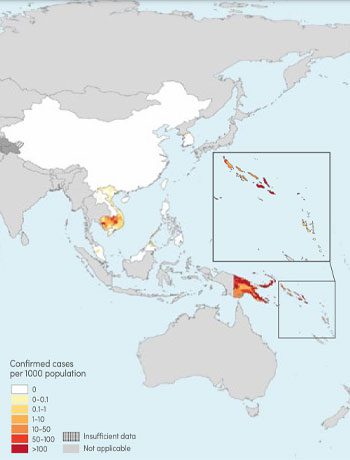
Source: World Health Organisation: World Malaria Report 2019 p.152, 154
You can find detailed malaria risk maps for every country on the Fitfortravel website. Click on the name of the country then on the “Malaria map”.
Young children and the elderly are at greater risk of contracting malaria and the effects can be more severe.
In pregnant women, malaria increases the rate of miscarriage and can lead to maternal death or delivery of low birth-weight infants.
According to the World Health Organisation, in 2018, there were 228 million cases of malaria and 405,000 deaths from malaria globally. Children aged under 5 years accounted for more than 60% of deaths.
Developing an effective vaccine could save hundreds of thousands of lives. However, it’s very difficult as the life cycle of the malaria parasite has many different stages.
In recent years, a lot of progress has been made in the search for a malaria vaccine. Several vaccines are currently being developed. The RTS,S/AS01 vaccine, developed with the support of the Bill and Melinda Gates Foundation, is now recommended for children at risk in some areas of the world. Source: World Health Organisation
At this particular moment in time there’s no vaccine available for travellers. Therefore, the only two ways to shield yourself from malaria are to protect yourself from mosquito bites and to take antimalarial medicine.
There’s no malaria vaccine for travellers yet
Prescribing preventative antimalarial treatment for long-term travellers is a medical procedure that needs to be personalised during a specialist consultation. Before leaving, rather than seeing your usual GP, make an appointment at a travel clinic (see the directory of travel clinics in the US and the UK).
Doctors there specialise in tropical diseases and can better advise you on whether or not you need to take preventative treatment depending on:
For long stays of several months in Asia or Latin America, some doctors will advise you against taking treatment.
This is because they consider the risk of undesirable side effects to be greater than the risk of malaria. Prevention methods vary greatly from one country to another. In Great Britain, Switzerland and Germany, for example, preventative treatment is no longer recommended in low risk areas.
According to a survey we carried out amongst 1,785 RTW travellers, only 32% of them took antimalarial treatment during their trip.
See our article on Vaccines for a Round-the-World Trip
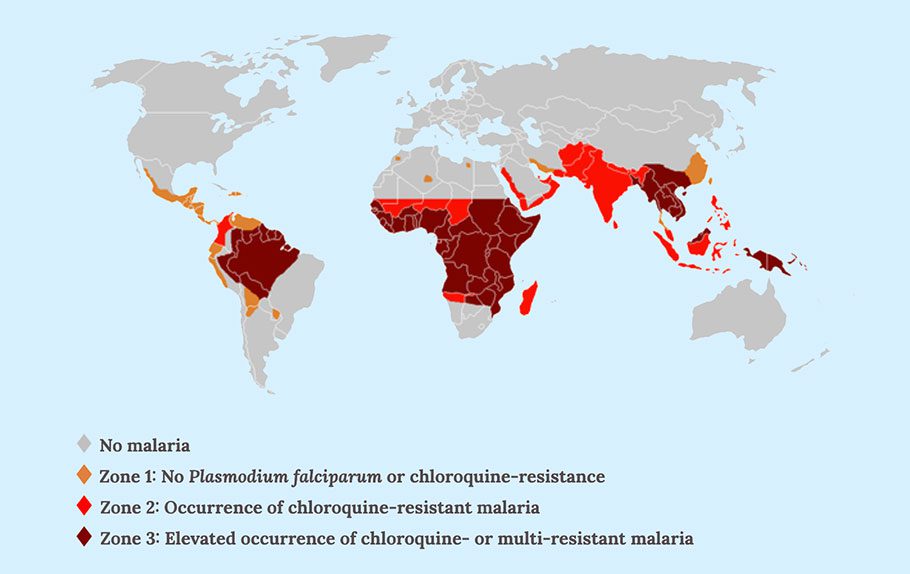
If you’re taking antimalarial treatment during your trip, the type of medication your doctor prescribes you will depend on the area you’re visiting. There are three major zones in the world, based on the level of resistance to chloroquine (one of the antimalarial drugs).
Chloroquine-resistant zones
What are the right antimalarials for each zone?
Here we specify the name of the drug with the trademark in brackets, as there are often cheaper generic (non-branded) versions.
Zone 1 :
Chloroquine (Avloclor® or Malarivon®)
Zone 2 :
Chloroquine + Proguanil (Avloclor® or Malarivon® + Paludrine®)
or Atovaquone and Proguanil (Malarone® or Maloff Protect®)
Zone 3 :
Atovaquone and Proguanil (Malarone® or Maloff Protect®)
or Mefloquine (Lariam®)
or Doxycycline (Vibramycin®)
Most RTW travellers go through Southeast Asia which is in zone 3. If you decide to take antimalarial treatment, you’ll therefore have to choose between Lariam®, Vibramycin® or Malarone®.
There’s a ban on sales of Lariam in many countries because of its neurological side effects which can sometimes be serious. So, if you’re travelling in zone 3, Doxycycline and Malarone are the other options.
Doxycycline has the advantage of being extremely cheap, but there are also several disadvantages:
Malarone is the drug with the fewest side effects. It’s the only preventative treatment that can also be used as emergency treatment in the event of infection (see below). It can’t be used for more than three months.
The Malarone brand is quite expensive, but you can now find the same drug in generic medication for a decent price.
Characteristics of each antimalarial drug
| Drug | Malarone® | Maloff Protect® | Vibramycin® | Avloclor® | Malarivon®Syrup | Lariam® | Paludrine® |
|---|---|---|---|---|---|---|---|
| Active Ingredients | Antovaquone + Proguanil | Antovaquone + Proguanil | Doxycycline | Chloroquine | Chloroquine | Mefloquine | Proguanil |
| Dosage | 1 tablet per day | 1 tablet per day | 1 tablet per day | 2 tablets per week | 1 dose per week (30ml) | 1 tablet per week | 2 tablets per day |
| First dose | 1 – 2 days before travel | 1 – 2 days before travel | 1 – 2 days before travel | 1 week before travel | 2 weeks before travel | 10 days before travel | 1 week before travel |
| Length of treatment | 7 days after leaving | 7 days after leaving | 4 weeks after leaving | 4 weeks after leaving | 4 weeks after leaving | 4 weeks after leaving | 4 weeks after leaving |
| Main side effects |
Headache
Stomach upset |
Headache
Stomach upset |
Light sensitivity: avoid too much exposure and protect yourself
from the sun.
Headache Stomach upset It’s an antibiotic. Usual disadvantages such as thrush, amongst others. Not recommended for pregnant women and children under the age of 8. |
Stomach upset
Visual disturbances (reversible) Skin reactions |
Headache
Stomach upset Insomnia Skin reactions |
Highly controversial drug. Some travellers don’t have side
effects, but for those who do, they can be extremely dangerous.
Neuropsychiatric disorders: convulsions, depression, anxiety, agitation, confusion, dizziness, which can lead to suicidal tendencies. |
Stomach upset
Mouth ulcers, inflammation of mouth mucous membranes. |
| Generic medication |
Yes See the list |
Yes See the list |
Yes See the list |
No | No | No | No |
| Price | around £50 for 16 branded tablets (1 week trip) and around £20 for 16 generic tablets | around £40 for 24 branded tablets (2 weeks trip) and around £20 for 16 generic tablets | around £38 for 30 dispersible tablets and around £12 for 37 generic tablets | around £12 for 20 tablets | around £12 for 60ml | around £23 for 8 tablets (1 week trip) | around £19 for 98 tablets |
It’s advised to avoid travelling in malaria risk areas with young children. However, children who weigh at least 25 lbs (11 kg) can take antimalarial medication.
Malarone is now available in pediatric tablets. Children who weigh at least 25 lbs (11 kg) can take it.
Dosage :
Doxycycline often isn’t prescribed for children under the age of 8.
Dosage :
It’s recommended to protect children against mosquitoes and to quickly consult a doctor if they have a temperature, or even plain discomfort for infants without a temperature.
Travelling in zone 3 isn’t recommended for pregnant women. However, if you still choose to go there, Malarone and Lariam can be prescribed, but Doxycycline can’t.
We’ve had several comments from readers who’ve seen the Malaria Business documentary which is about Artemisia annua. According to this documentary, this plant, which has been used in Chinese medicine for many years, contains artemisinin which can be used to treat malaria.
We urge you to be careful: in some forms, it can be used to treat malaria, but not to prevent it.
The World Health Organisation strongly recommends the use of combination therapies based on artemisinin to treat certain mild forms of malaria. However, the WHO doesn’t recommend the use of Artemisia annua herbal teas for the prevention and treatment of malaria because the amount of artemisinin in it isn’t enough. One litre of Artemisia annua infusion only contains 20%, at most, of the dose of artemisinin in a drug.
Antimalarial treatments don’t guarantee full protection. Whether you take them or not, it’s therefore very important to protect yourself from mosquito bites to avoid contracting malaria, as well as other tropical diseases such as dengue, yellow fever, zika or chikungunya.
How to protect yourself from mosquitoes:

A plug-in mosquito repellent is less cumbersome than a mosquito net.
We always think twice about putting chemical products on our skin. That’s why we see lots of alternative solutions popping up on the market: essential oil bracelets, citronella candles, herbal extract sprays, UV lamps, ultrasonic devices and even smartphone apps. However, a group of biologists at the New Mexico State University conducted tests and concluded that not all of these solutions are effective.
The only products that are actually efficient are made from:
See the New Mexico State University’s study in detail
The maximum recommended concentration level differs depending on the product and the age of the person using the repellent, as well as for pregnant women. So check the concentration of a product before buying it.
Concentration and maximum number of applications of different repellents
| Age |
Maximum number of applications per day |
DEET | Picaridin | Citridiol | IR3535 |
|---|---|---|---|---|---|
| 6 months – walking age | 1 | 10% – 30% | – | 20% – 30% | 20% |
| Walking age – 24 months | 2 | 10% – 30% | 20% – 30% | 20% | |
| 24 months – 12 years | 2 | 20% – 30% | 20% – 30% | 20% – 30% | 20% – 35% |
| > 12 years | 3 | 20% – 50% | 20% – 30% | 20% – 30% | 20% – 35% |
| Pregnant woment | 3 | 30% | 20% | 20% | 20% |
If you have a fever for more than 24 hours during your trip or within three months of your return, see a doctor urgently.
A blood test will need to be done to determine if it’s malaria, as many other tropical diseases have the same symptoms.
If you plan on travelling in extremely remote areas, you can ask your doctor to prescribe emergency treatment that you can take with you. This self-treatment should only be taken if you can’t get a doctor’s appointment within 24 hours of the onset of the fever. In any case, you’ll need to see a doctor as soon as possible afterwards to check that it’s not another disease.
Emergency treatment shouldn’t be used:
Drugs that can be used in emergency treatment are:
Halofantrine (Halfan®) shouldn’t be prescribed due to its potential cardiovascular toxicity.



